If you’re a male runner over 50 and you’ve never checked your DHEA-S, there’s a good chance it’s low.
Not because something is wrong with you. Not because your adrenal glands are failing. But because the running you’re doing for your health may be one of the primary reasons it’s suppressed.
This surprises most people. We assume that fitter means hormonally younger — and in many ways, that’s true. VO2max, insulin sensitivity, resting heart rate, mitochondrial density: all trend younger in trained runners. But DHEA-S is one marker where chronic high-mileage training actively works against you, and it’s worth understanding why.
What DHEA-S Actually Is
DHEA (dehydroepiandrosterone) is a steroid hormone produced primarily by the adrenal cortex, specifically a layer called the zona reticularis. DHEA-S is its sulfated form — the version that circulates in blood and gets measured on a standard lab panel. It’s the most abundant circulating steroid hormone in the human body during your 20s and 30s, and it declines with age at a predictable rate, dropping roughly 2–3% per year after age 30.
DHEA sits high in the steroidogenesis pathway. It’s a prohormone — it gets converted downstream into other hormones: androstenedione, testosterone, and estrogens, depending on what your tissue-level enzymes do with it. It also acts directly on its own receptors in the brain, immune system, and bone, independent of those downstream conversions.
When DHEA-S is low, it’s not just a number on a report. It represents a compressed upstream substrate pool for multiple hormonal pathways simultaneously.
The Normal Decline After 50 — and Why Runners Drop Further
By age 50, most men have already lost 50–60% of their peak DHEA-S. That’s just biology. The zona reticularis atrophies with age, independent of anything else you’re doing.
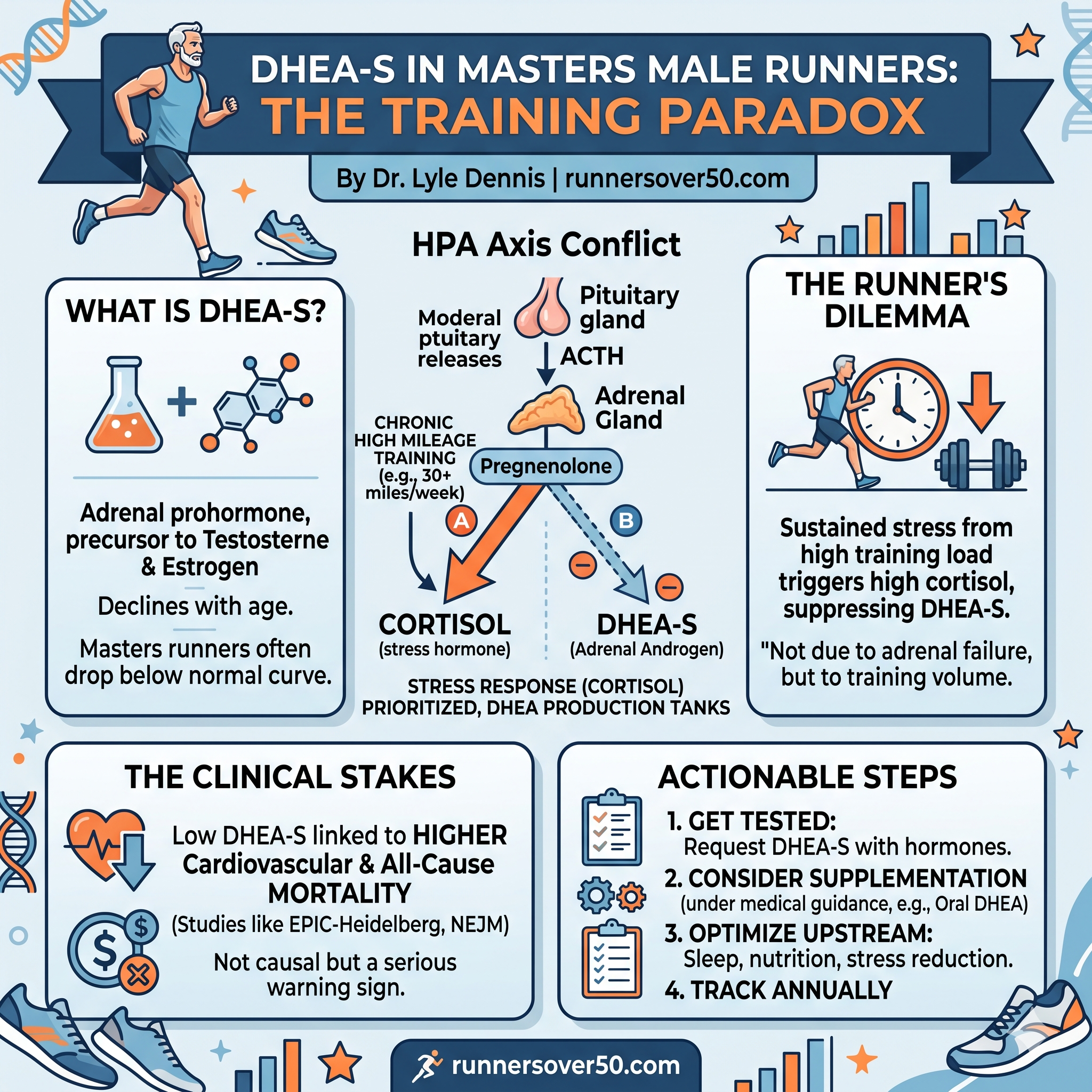
But endurance runners don’t just follow the normal decline curve. They tend to fall significantly below age-matched sedentary peers. The reason comes down to the HPA axis and a matter of competing priorities.
DHEA and cortisol share the same upstream precursor: pregnenolone. When the adrenal gland needs to choose between producing cortisol and producing DHEA, cortisol wins. It’s the stress hormone. It’s metabolically urgent. DHEA is downstream and deferrable.
Chronic high-mileage running is a sustained stressor on the HPA axis. Not in a pathological sense — the adaptations it drives are profoundly positive. But from your adrenal gland’s perspective, 30+ miles a week at moderate-to-hard effort is a chronic demand signal. ACTH — the pituitary hormone that drives the adrenals — gets chronically elevated in response to training load, and ACTH preferentially drives cortisol synthesis over DHEA.
The result: long-term endurance athletes consistently show lower DHEA-S than age-matched non-athletes. This is one of the more counterintuitive findings in masters athlete physiology, and most runners — and many physicians — don’t know it.
The Clinical Stakes
Why does this matter beyond a number on a lab report?
The EPIC-Heidelberg prospective cohort study — one of the largest observational studies on DHEA-S and mortality — followed over 9,000 men and found a clear relationship between DHEA-S levels and mortality risk. Men in the lowest quintile for their age had 83% higher cardiovascular mortality, 27% higher cancer mortality, and 51% higher all-cause mortality compared to men in the middle quintile.
In the continuous analysis, every doubling of DHEA-S below the median was associated with approximately 14% lower cardiovascular mortality.
Earlier work by Barrett-Connor and colleagues, published in the New England Journal of Medicine, found that men with DHEA-S below roughly 140 µg/dL had a cardiovascular disease mortality hazard ratio of approximately 3.3 compared to men above that threshold.
These are observational associations, not causal proofs. Men with low DHEA-S may have other underlying conditions driving both the low hormone and the elevated mortality risk. But the biological mechanisms are plausible: DHEA has anti-glucocorticoid properties, direct immune-modulatory effects, roles in bone maintenance, and indirect androgenic effects via downstream conversion to testosterone.
For a runner already exercising for longevity, landing in the lowest DHEA-S quintile for your age — potentially as a direct consequence of the training you’re doing for health — is a genuine irony worth taking seriously.
Other Contributing Factors
Endurance training is likely the dominant driver in a masters male runner with low DHEA-S, but it’s rarely the only factor:
Age-related zona reticularis decline. This happens to everyone. High training volume compounds an already-declining baseline.
Chronic psychological stress. The same cortisol-dominance mechanism that training triggers applies to non-training stress. A high-demand life stacked on top of high training load worsens the pregnenolone allocation problem.
Prior hormonal therapy. Men who have used testosterone replacement therapy may have partially suppressed adrenal androgen output during that period. Recovery takes time after discontinuation.
Genetics. Some men have lower adrenal DHEA output as a constitutional trait — variation in enzymes like SULT2A1 (which governs sulfation of DHEA into DHEA-S) influences baseline levels independently of training or age.
What to Do About It
This is not a call to stop running. The longevity benefits of consistent high mileage — VO2max preservation, cardiovascular remodeling, metabolic efficiency, neuroplasticity, bone density — almost certainly outweigh the DHEA-S suppression. You don’t solve the problem by eliminating the cause.
Get the number first. A standard metabolic panel won’t include DHEA-S. You have to ask for it. Request it alongside morning cortisol, free and total testosterone, and estradiol. This gives you a hormonal picture, not just a single data point.
Consider supplementation with your physician. Oral DHEA at 25–50mg daily is the most studied approach. Because DHEA is a prohormone, it converts downstream — modest increases in testosterone and estradiol are possible and should be monitored. A recheck of DHEA-S, testosterone, estradiol, hematocrit, and PSA at 8–12 weeks is reasonable. Individual response is highly variable.
Optimize upstream. Ensure you’re not compounding the problem: chronic sleep debt, inadequate caloric intake for your training load, and excessive caffeine all worsen cortisol burden and tighten the pregnenolone squeeze.
Track it annually. A single low value is a snapshot. Trending DHEA-S year over year — and watching how it responds to any intervention — gives you a dynamic picture.
The Bottom Line
DHEA-S declining with age is normal. DHEA-S declining faster because you’re logging high miles is an underrecognized consequence of the training we do for longevity. The same HPA axis activation that drives beneficial adaptations in the cardiovascular system suppresses adrenal androgen output over time.
If you’re a masters male runner and you’ve never checked your DHEA-S, check it. If it’s low, don’t assume it’s just age. Your training may be a primary cause — and there are things you can do about it.